Here is the referto of the MRI. See the key point is that there is contusion but not detectable ischemia (suspected some small areas of ischemia somewhere). The effects should be temporary.
Also Dr Veneziani says the bruised area has no known function -- when it is removed to remove a tumor, there are no known effects.
So very good
 my effort to translate
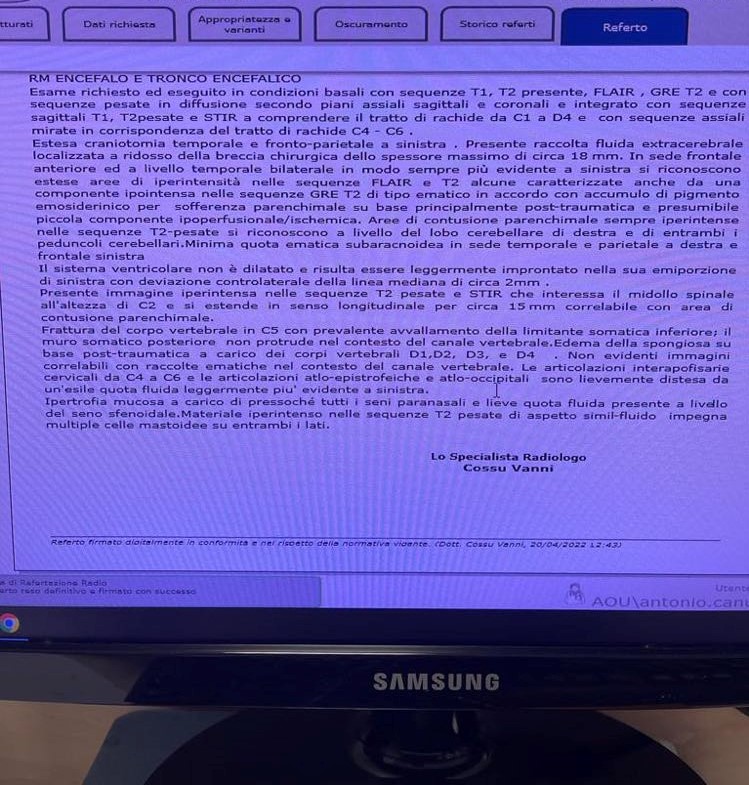
Exam rquested and executed in basal conditions with sequence t1,t2,presente, flair, GRE T2 amd with sequences weighed in diffusion according to axial, sagitale and coronal axes and with an axial sequence aiming in correspondende to the “tratto di rachide” C-4-C6
Extensive craniotomy temporal and fronto- parietal on the left. A collection of extracerebrale fluid collected near the surgical breach of maximum thickness of 18mm. Frontal and temporal bilaterally (walways more evident on the left, there is an extensive area of hyperintensity in the FLAIR and T2 sequences with some characteristics also of a hypointense component in the GRE T2 sequence of a hematic type in agreement with the accumulation of hemo siderinic pigment due to parenchimal suffering of a base which is principally post-traumatic and presumably a small component that is hypofusional/ischemic. Area of parenchimal contusion always hyperintense in the T2-weighed sequence are recognized at the level of the right cerebellar lobe and both cerebellar [penducoli]. Minimal subaracnoide hematic level in the temporal and parietal areas on the right and the left frontal area.
The ventricular system is not dilated and is lightly [improntato] (printed ???) in its left hemiportion with centrolateral deviation of the median line of roughly 2 mm.
There is a hyperintense area in the T2 weighted sequence and STIR that involves the spinal medulla at the level of C2 and which extends in a longitudinal direction for roughly 15 mm correlatable with the area of parenchimal contusion.
The corpo (bit part also called soma or maybe body) of the C5 vertebra is fractured pricinpally related to the lower somatic [limitante]. The posterior somatic wall does NOT protrude in the context of the vertebral canal. Edema of the “spongiosa” of a post traumatic sort affecting the vertebral “corpi – big parts soma whatever) of D1 D2 D3 and D4. No evidence of hematic accumulation (I think that means “blood”) in the context of the vertebral canal. The “interapofisary” joints of c4 and c6 and the “atio epitrophic” and “atio-occipital’ joints are slightly spread by a tiny amount of fluid which is slightly more evident on the left.
Mucosal hypotophy of almost all of the paranasal “seni” (I think sinuses) and a small quota of fluid present at the level of the Sphenodale “seno” (I think sinus). Hyper intense material in the T2 weighted sequence of a fluid like appearance involves many “celle mastoidee” on both sides.
my effort to translate
Exam rquested and executed in basal conditions with sequence t1,t2,presente, flair, GRE T2 amd with sequences weighed in diffusion according to axial, sagitale and coronal axes and with an axial sequence aiming in correspondende to the “tratto di rachide” C-4-C6
Extensive craniotomy temporal and fronto- parietal on the left. A collection of extracerebrale fluid collected near the surgical breach of maximum thickness of 18mm. Frontal and temporal bilaterally (walways more evident on the left, there is an extensive area of hyperintensity in the FLAIR and T2 sequences with some characteristics also of a hypointense component in the GRE T2 sequence of a hematic type in agreement with the accumulation of hemo siderinic pigment due to parenchimal suffering of a base which is principally post-traumatic and presumably a small component that is hypofusional/ischemic. Area of parenchimal contusion always hyperintense in the T2-weighed sequence are recognized at the level of the right cerebellar lobe and both cerebellar [penducoli]. Minimal subaracnoide hematic level in the temporal and parietal areas on the right and the left frontal area.
The ventricular system is not dilated and is lightly [improntato] (printed ???) in its left hemiportion with centrolateral deviation of the median line of roughly 2 mm.
There is a hyperintense area in the T2 weighted sequence and STIR that involves the spinal medulla at the level of C2 and which extends in a longitudinal direction for roughly 15 mm correlatable with the area of parenchimal contusion.
The corpo (bit part also called soma or maybe body) of the C5 vertebra is fractured pricinpally related to the lower somatic [limitante]. The posterior somatic wall does NOT protrude in the context of the vertebral canal. Edema of the “spongiosa” of a post traumatic sort affecting the vertebral “corpi – big parts soma whatever) of D1 D2 D3 and D4. No evidence of hematic accumulation (I think that means “blood”) in the context of the vertebral canal. The “interapofisary” joints of c4 and c6 and the “atio epitrophic” and “atio-occipital’ joints are slightly spread by a tiny amount of fluid which is slightly more evident on the left.
Mucosal hypotophy of almost all of the paranasal “seni” (I think sinuses) and a small quota of fluid present at the level of the Sphenodale “seno” (I think sinus). Hyper intense material in the T2 weighted sequence of a fluid like appearance involves many “celle mastoidee” on both sides.
Comments
Post a Comment